Guidelines and considerations for PBC management
When should second-line treatment for PBC be considered?
AASLD and EASL guidelines recommend assessing biochemical response to UDCA at 1 year.1,2
Evolving trends support that response to UDCA may be reliably predicted at 6 months, allowing for earlier consideration of second-line therapy.3-7,a
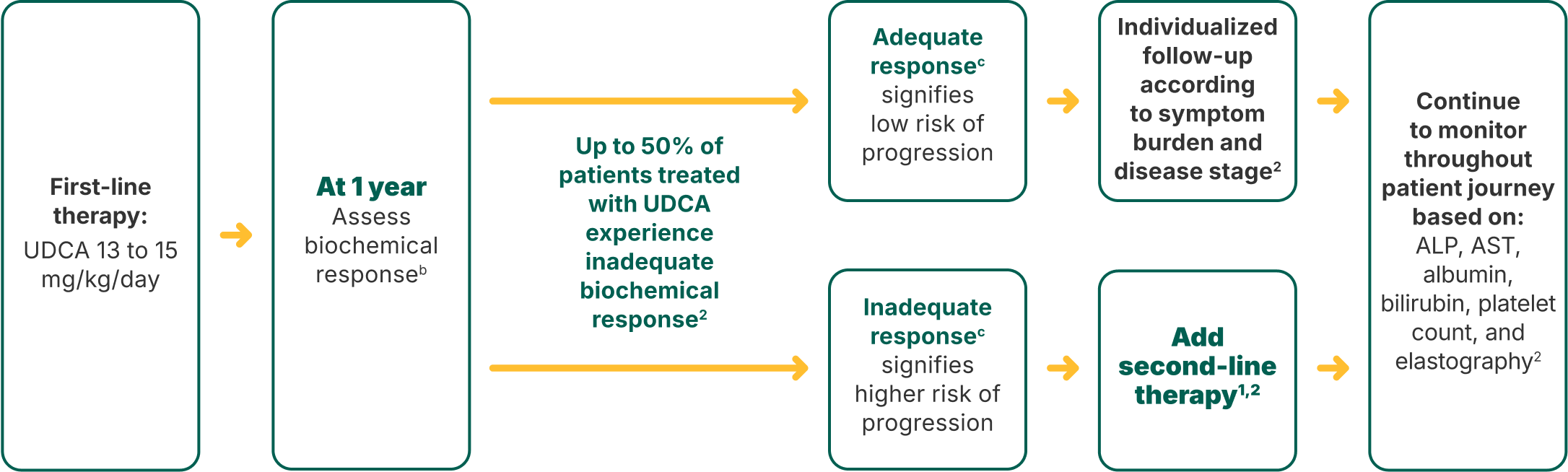
Current AASLD (2018) and EASL (2017) PBC treatment guidelines for patients on first-line UDCA treatment (adapted)1,2
First-line therapy: UDCA 13 to 15 mg/kg/day
At 1 year
Assess biochemical responseb
Adequate responsec
signifies low risk of progression
Inadequate responsec
signifies higher risk of progression
Individualized follow-up according to symptom burden and disease stage2
Add second-line therapy1,2
Continue to monitor throughout patient journey based on:
ALP, AST, albumin, bilirubin, platelet count, and elastography2
Swipe left to review
Evolving trends in second-line treatment evaluation
Target ALP normalization as a treatment goald
as suggested by a 2020 analysis of the GLOBAL PBC Study Group database (N=3059)8,e
At 6 months
The PBC Integrated Patient Care Pathway (2022) and a recently proposed treatment paradigm (2023) support growing evidence that response to first-line therapy may be reliably predicted at 6 months, allowing earlier consideration for second-line therapy3-6,a
- ALP and TB improvements are typically seen within a few weeks of initiating UDCA, and 90% of the improvement usually occurs within 6 to 9 months
- Assess patients for risk of progression
aAn updated expert consensus (2023) recommends a 6-month threshold of ALP <1.9 x ULN + bilirubin <1.0 x ULN in patients with advanced fibrosis (VCTE or TE ≥10 kPa), compensated liver disease, and no portal hypertension, and to continue monitoring ALP and bilirubin every 3 to 6 months with an adequate response to UDCA.5
bAn ALP-only criterion of ALP ≤1.67 x ULN can be used to assess biochemical response after 12 months of first-line therapy. Use other biochemical response criteria per clinical judgment.2
cNote that symptoms of PBC do not typically improve with UDCA monotherapy.1,3
dEach laboratory has its own set of reference ranges for ALP that may be divided according to age and gender. Commonly used labs suggest a normal ALP in the 42-125 IU/L range. Please consult the lab you use for its reference ranges.9
eThe primary endpoint was a composite of liver transplant and all-cause mortality. All patients in the study had normal bilirubin at baseline or 1 year. Normalization conclusion was based on a subgroup analysis of patients (n=1523) with ALP ≤1.67 x ULN who had normal bilirubin for 1 year.8



AASLD=American Association for the Study of Liver Diseases; ALP=alkaline phosphatase; AST=aspartate aminotransferase; EASL=European Association for the Study of the Liver; PBC=primary biliary cholangitis; TB=total bilirubin; TE=transient elastography; UDCA=ursodeoxycholic acid; ULN=upper limit of normal; VCTE=vibration-controlled transient elastography.
Tap for Important Safety Information, including warnings for fractures, liver test abnormalities, and biliary obstruction
LIVDELZI is indicated for the treatment of primary biliary cholangitis (PBC), in combination with ursodeoxycholic acid (UDCA) in adults who have had an inadequate response to UDCA, or as monotherapy in patients unable to tolerate UDCA.
This indication is approved under accelerated approval based on a reduction of alkaline phosphatase (ALP). Improvement in survival or prevention of liver decompensation events have not been demonstrated. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trial(s).
Limitation of Use: Use of LIVDELZI is not recommended in patients who have or develop decompensated cirrhosis (eg, ascites, variceal bleeding, hepatic encephalopathy).
IMPORTANT SAFETY INFORMATION
Warnings and Precautions
- Fractures: Fractures occurred in 4% of LIVDELZI-treated patients compared to no placebo-treated patients. Consider the risk of fracture in the care of patients treated with LIVDELZI and monitor bone health according to current standards of care.
- Liver Test Abnormalities: LIVDELZI has been associated with dose-related increases in serum transaminase (AST and ALT) levels >3x ULN in patients receiving 50 mg and 200 mg once daily (5x and 20x higher than the recommended dosage of 10 mg once daily). Perform baseline clinical and laboratory testing when starting LIVDELZI and monitor thereafter according to routine patient management. Interrupt treatment if the liver tests (ALT, AST, total bilirubin, and/or ALP) worsen, or if the patient develops signs and symptoms of clinical hepatitis (eg, jaundice, right upper quadrant pain, eosinophilia). Consider permanent discontinuation if liver tests worsen after restarting LIVDELZI.
- Biliary Obstruction: Avoid use of LIVDELZI in patients with complete biliary obstruction. If biliary obstruction is suspected, interrupt LIVDELZI and treat as clinically indicated.
Adverse Reactions
- The most common adverse reactions (≥5%) with LIVDELZI were headache (8%), abdominal pain (7%), nausea (6%), abdominal distension (6%), and dizziness (5%).
Drug Interactions
Potential Increased Exposure of LIVDELZI with:
- Probenecid: Avoid coadministration with LIVDELZI.
- Strong CYP2C9 Inhibitors: Monitor for adverse effects during concomitant use.
- Dual Moderate CYP2C9 and Moderate or Strong CYP3A4 Inhibitors (eg, fluconazole): Monitor for adverse effects during concomitant use.
- CYP2C9 Poor Metabolizers Using Moderate or Strong CYP3A4 Inhibitors: Monitor for adverse effects during concomitant use of a moderate or strong CYP3A4 inhibitor in patients who are CYP2C9 poor metabolizers.
- Dual or Multiple Clinical Inhibitors of Drug Transporters OATP1B1, OATP1B3, and BCRP (eg, cyclosporine): Monitor for adverse effects during concomitant use.
Potential Reduction in LIVDELZI Exposure with:
- Rifampin: Concomitant use of LIVDELZI with rifampin, an inducer of metabolizing enzymes, may result in delayed or suboptimal LIVDELZI biochemical response. Monitor biochemical response (eg, ALP and bilirubin) when patients initiate rifampin during LIVDELZI treatment.
- Bile Acid Sequestrants: Administer LIVDELZI at least 4 hours before or 4 hours after taking a bile acid sequestrant, or at as great an interval as possible.
Pregnancy and Lactation
- Pregnancy: There are insufficient data from human pregnancies exposed to LIVDELZI to allow an assessment of a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Report pregnancies to Gilead Sciences, Inc., at 1-800-445-3235.
- Lactation: There are no data on the presence of LIVDELZI in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for LIVDELZI and any potential adverse effects on the breastfed infant from LIVDELZI.
Please see full Prescribing Information for LIVDELZI.
References
-
- Lindor KD, Bowlus CL, Boyer J, Levy C, Mayo M. Primary biliary cholangitis: 2018 practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019;69(1):394-419. doi:10.1002/hep.30145
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: the diagnosis and management of patients with primary biliary cholangitis. J Hepatol. 2017;67(1):145-172. doi:10.1016/j.jhep.2017.03.022
- Murillo Perez CF, Ioannou S, Hassanally I, et al; GLOBAL PBC Study Group. Optimizing therapy in primary biliary cholangitis: alkaline phosphatase at six months identifies one-year non-responders and predicts survival. Liver Int. 2023;43(7):1497-1506. doi:10.1111/liv.15592
- Kowdley KV, Bowlus CL, Levy C, et al. Application of the latest advances in evidence-based medicine in primary biliary cholangitis. Am J Gastroenterol. 2023;118(2):232-242. doi:10.14309/ajg.0000000000002070
- Hirschfield GM, Chazouillères O, Cortez-Pinto H, et al. A consensus integrated care pathway for patients with primary biliary cholangitis: a guidelines-based approach to clinical care of patients. Expert Rev Gastroenterol Hepatol. 2021;15(8):929-939. doi:10.1080/17474124.2021.1945919
- Levy C, Bowlus CL. Primary biliary cholangitis: personalizing second-line therapies. Hepatology. 2025;82(4):895-910. doi:10.1097/hep.0000000000001166
- Invernizzi P, Floreani A, Carbone M, et al. Primary biliary cholangitis: advances in management and treatment of the disease. Dig Liver Dis. 2017;49(8):841-846. doi:10.1016/j.dld.2017.05.001
- Murillo Perez CF, Harms MH, Lindor KD, et al; GLOBAL PBC Study Group. Goals of treatment for improved survival in primary biliary cholangitis: treatment target should be bilirubin within the normal range and normalization of alkaline phosphatase. Am J Gastroenterol. 2020;115(7):1066-1074.
- Labcorp. Alkaline phosphatase. Accessed May 7, 2025. https://www.labcorp.com/tests/001107/alkaline-phosphatase